Background. Gingival recession in its localized or generalized form is an undesirable
condition resulting in root exposure.The result often is not esthetic and may lead to sensitivity and root caries. Exposed root surfaces also are prone to abrasion. The purpose of this article is to describe the prevalence, etiology and factors associated with gingival recession.
Types of Studies Reviewed. The authors reviewed cross-sectional epidemiologic studies of gingival recession and found that they correlated the prevalence of recession to trauma, sex, malpositioned teeth,
inflammation and tobacco consumption. The recent surveys they reviewed revealed that 88 percent of people 65 years of age and older and 50 percent of people 18 to 64 years of age have one or more sites with
recession. The presence and extent of gingival recession also increased with age.
Results. More than 50 percent of the population has one or more sites with gingival
recession of 1 mm or more. The prevalence of gingival recession was found in patients with both good and poor oral hygiene. It has been proposed that recession is multifactorial, with one type being associated with
anatomical factors and another type with physiological or pathological factors. Recession has been found more frequently on buccal surfaces than on other aspects of the teeth.
Clinical Implications. Dentists should be knowledgeable about the etiology, prevalence and associating factors of gingival recession, as well as treatment options, so that appropriate treatment modalities can be offered to patients. Treatments for gingival recession include gingival grafting, guided tissue regeneration and orthodontic therapy. Such treatments typically result in esthetic improvement, elimination of sensitivity and a decreased risk of developing root caries.
Gingival recession is characterized by the displacement of the gingival margin apically from the
cementoenamel junction, or CEJ, or from the former location of the CEJ in which restorations have distorted the location or appearance of the CEJ. Gingival recession can be localized or generalized and be associated with one or more surfaces.(Smith RG. 1997) The resulting root exposure is not esthetically
pleasing and may lead to sensitivity and root caries. As a result, we reviewed studies that described the prevalence, etiology and factors associated with gingival recession.
AGING
Similarly, Gorman found that the frequency of gingival recessio increased with age and was greater
in men than in women of the same age. Malpositioned teeth and toothbrush trauma were found to be the
most frequent etiologic factors associated with gingival recession.
Recession associated with labially positioned teeth occurred in 40 percent of patients 16 to 25 years of age
and increased to 80 percent of patients in the 36 to 86 years of age group. Those findings were corroborated
by Murray, who examined 4,000 subjects and found that the incidence of gingival recession increased with age.
ANATOMICAL FACTORS
One etiologic factor that may be associated with gingival recession is a prior lack of alveolar bone
at the site. The deficiencies in alveolar bone may be developmental (anatomical) or acquired (physiological
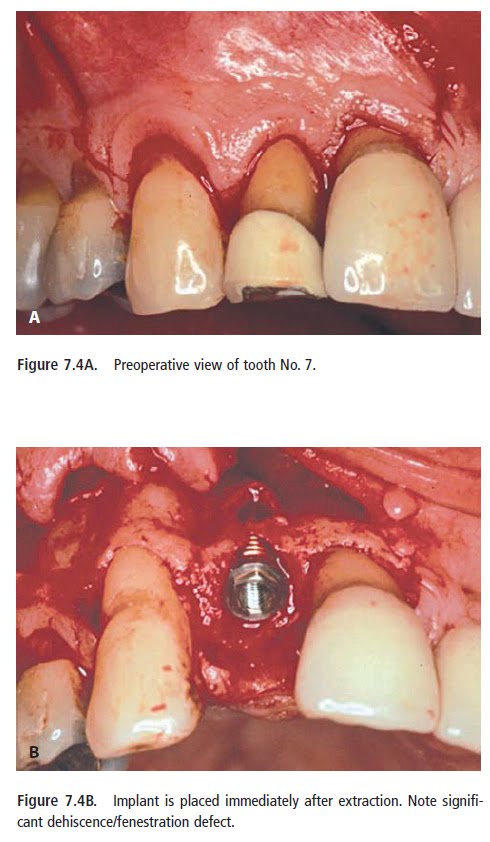
or pathological).Anatomical factors that have been related to recession include fenestration and dehiscence of
the alveolar bone, abnormal tooth position in the arch, aberrant path of eruption of the tooth and
individual tooth shape. All those anatomical factors are interrelated and may result in an alveolar
osseous plate that is thinner than normal and that may be more susceptible to resorption.
PHYSIOLOGICAL FACTORS
Physiological factors may include the orthodontic movement of teeth
to positions outside the labial or lingual alveolar plate, leading to dehiscence formation.Such
studies suggested that the acquired loss of alveolar bone might be associated with a number of identifiable
physiological or pathological conditions for which bone loss is part of a physiological or pathological
process.
PATHOLOGICAL FACTORS
Pathological factors include bone resorption as a sequel to microbially induced periodontal diseases.
In this case, however, the process of recession may be more complex since the teeth
involved may extrude, tilt and become mobile. A rat study demonstrated a possible mechanism of
gingival recession, showing that loss of attachment was the result of localized inflammatory
processes in connective tissue with the accumulation of mononuclear cells.(Baker DL 1976) It also was suggested that inflammation may persist subclinically and therefore cannot be eliminated as a factor in
recession.Similarly, recession has been related to inflammation in periodontal connective tissue
in monkeys.(Hopps 1974)
TRAUMA
In addition to psychological factors, various forms of trauma—such as vigorous toothbrushing, aberrant
frenal attachment, occlusal injury, operative procedures and tobacco chewing—have been thought to play a role in the etiology of recession.
Traumatic mechanical toothbrushing is factor in the etiology of gingival recession. The effects of toothbrushing have been studied by many investigators with general agreement that vigorous or incorrect use of the toothbrush can produce recession.
HYGIENE
The frequency of gingival recession in subjects with excellent oral hygiene has been reported to
be more frequent at buccal than proximal or lingual surfaces. In an epidemiologic study, gingival
recession was positively correlated with the frequency of toothbrushing.
Recession occurs more frequently in patients with good rather than poor oral hygiene.(O’Leary TJ 1971)
ABERRANT FRENAL ATTACHMENT
Aberrant frenal attachment also has been mentioned as a cause of localized
recession, but the evidence is not overwhelming. Some studies did not find any correlation
between frenal pull and recession, whereas thers did find an association.
CLASSIFICATION SYSTEMS
The Miller classification system.
A. Class I recession. B. Class II recession. C. Class III recession. D. Class IV recession.
TREATMENT OPTIONS
Different gingival grafting techniques have been proposed to treat gingival recession, including the lateral sliding flaps, coronally positioned flaps and connective tissue grafts, resulting in mean
root coverage of 65 to 98 percent. Guided tissue regeneration was introduced later to treat
recession, using bioabsorbable or nonabsorbable membranes, and studies showed similar results
with a mean root coverage of 48 to 92 percent. Orthodontic treatment can be considered with or
without periodontal surgery, especially in situations were teeth are malpositioned.
The etiology and prevalence of gingival recession
MOAWIA M. KASSAB, D.D.S., M.S.; ROBERT E.COHEN, D.D.S., Ph.D.
J Am Dent Assoc 2003;134;220-225
About different treatment techniques of gingival recession we will talk at future posts.