Human mineralized bone in extraction sites before implant placement
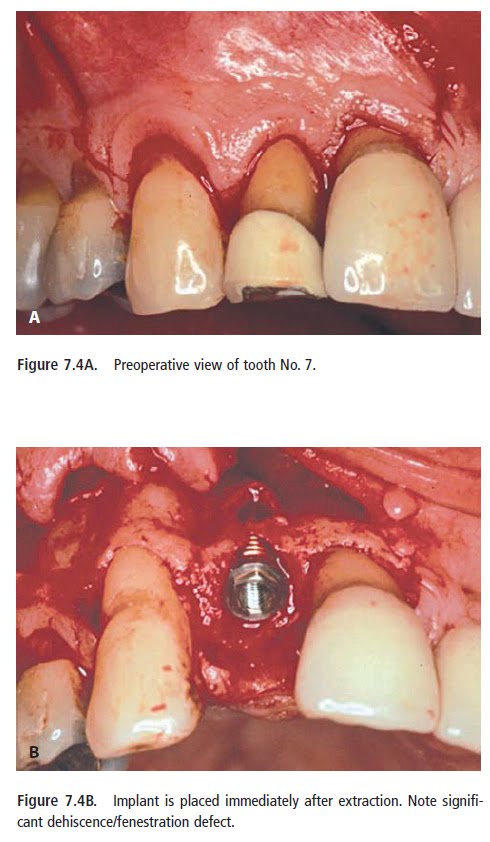
After tooth extraction, labial or facial bone loss may be significant, resulting in less-thanideal
bone being available for implant placement. Horizontal or vertical deficiency with
loss of interseptal, mesial or distal bone also may occur, depending on the etiology
leading to tooth extraction, such as severe periodontal disease or chronic
bone loss from tooth fracture. Even after a “clean” extraction, bone loss may be
unpredictable, resulting in limitation of ideal implant placement.
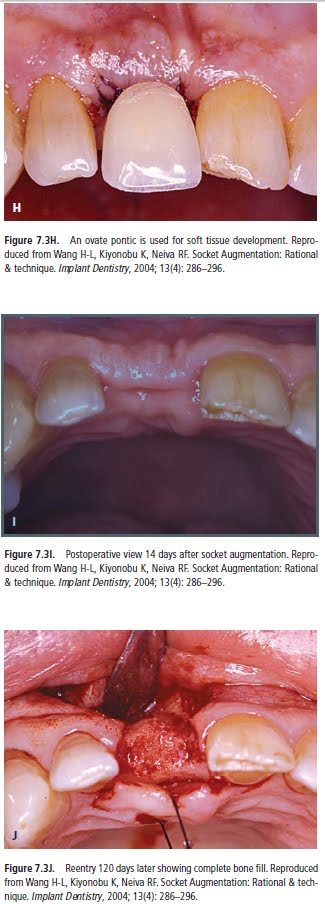
Major changes of an extraction site take place during the 12 months following tooth extraction. The width of the alveolar ridge was reduced by 50% during the observation period (12 months). This loss, corresponding to 5 to 7 mm, is in agreement with earlier studies. The finding that approximately two thirds of this reduction occurred within the first 3 months after tooth extraction also corresponds to earlier findings.(Lars Schropp, 2003)
In an effort to preserve and create sufficient bone for implant placement after mandibular molar extraction, we have used human mineralized cancellous bone (Puros, Sulzer Dental, Carlsbad, Calif.) as a graft material. For mandibular molar sites, we have used advancement flaps to achieve primary closure, without the use of membranes or collagen. This technique has allowed
for successful placement of implants in molar sites that otherwise may not have had satisfactory amounts of bone for ideal implant placement.
Background. Bone loss after tooth extraction may prevent dental implant placement. Human mineralized bone grafts can be used to restore bone volume and allow for tooth replacement with dental implants.
Methods. The authors grafted 22 sites in 18 patients with human mineralized bone after tooth extraction. They allowed molar sites 16 weeks for graft healing, placed the implants
and restored them with a final crown after a four-month integration period. Singlerooted
maxillary sites received implants and immediate placement of provisional crowns or underwent a delayed two-stage restoration approach. The authors used radiographs and clinical examinations to evaluate the results.
Results. All of the sites were restored successfully with a single-tooth implant restoration.
Periapical radiographs indicated that the crestal bone levels were limited to
the first thread of the implants or slightly coronal to the first thread of the implant.
Clinical evaluation indicated excellent gingival health around the provisional and
final restorations, without obvious gingival migration.
Conclusions. The use of human mineralized bone may have significant potential to
reconstruct missing bone resulting from tooth extraction and to preserve bone after
tooth extraction. In addition, healed bone graft sites seem to be able to support immediate
placement of a provisional crown and implant restorations.
Clinical Implications. Patients who are having teeth extracted may become candidates
for implant restorations when the sites are appropriately grafted to preserve and reconstruct bone volume, thus allowing for more options for reconstructing the
missing tooth site.
CASE PRESENTATION
MICHAEL S. BLOCK, D.M.D.; ISRAEL FINGER, D.D.S.,
ROBERT LYTLE, D.D.S.
J Am Dent Assoc 2002;133;1631-1638